Recent posts on this blog focused on generating synthetic healthcare data both using Claude for greenfield work, When There's No Schema... and using Snowflake, Generating Synthetic Data In Snowflake. Useful plumbing, but plumbing is only interesting because of what runs through it.
This post is about what we built on top of that plumbing.
We call it Axiom - the High-Risk Patient Command Center. We developed this reference application to show the power of a value-based care workflow with a modern data-stack and built-in AI assistance. Everything below runs on enterprise grade technologies, and on the kind of synthetic clinical data those earlier posts produce.
The problem Axiom is built around
Picture a care manager. Their job is to work through a patient population, find the people at highest risk of a negative and expensive outcome, and mitigate the situation before it happens.
In practice that job is a tab-switching marathon. Population analytics live in one tool. The patient-level data lives in another. The care plan lives in a third. Risk scores, if they exist at all, live in a data science notebook nobody in the clinic can open. By the time you've assembled a picture of a single high-risk patient, you've touched five systems and an hour is gone — and you have a patient population of fourteen thousand to tend to.
Axiom collapses that into one workflow. AI-assisted insights and actions sit next to embedded analytics, both built on a cutting-edge data stack, and the care manager gets a single front door to their day.
The rest of this post walks the workflow the way we walk it in a live demo: population down to a single patient's next action — and then shows how it's assembled.
What it's built on
Four core "best of breed" technologies:
- Omni Analytics: embedded, interactive dashboards and the out-of-the-box analytics experience, including its native chatbot, Blobby.
- Snowflake Cortex: the AI/ML layer. Risk classification, readmission probability, and anomaly detection over the population.
- dbt: the transformation layer that turns raw healthcare data into clean, analytics-ready models.
- The Tuva Project: open-source dbt packages for healthcare: clinical concepts, condition groupers, HEDIS measures, and the readmission logic the risk models lean on.
Astrodata's contribution is the integration layer that makes these feel like one product, plus the Axiom agent — the piece that turns findings into actions. More on the two-agent idea in a moment, because it's the part that makes this more than a pretty dashboard.
Step 1 — Population Health Intelligence
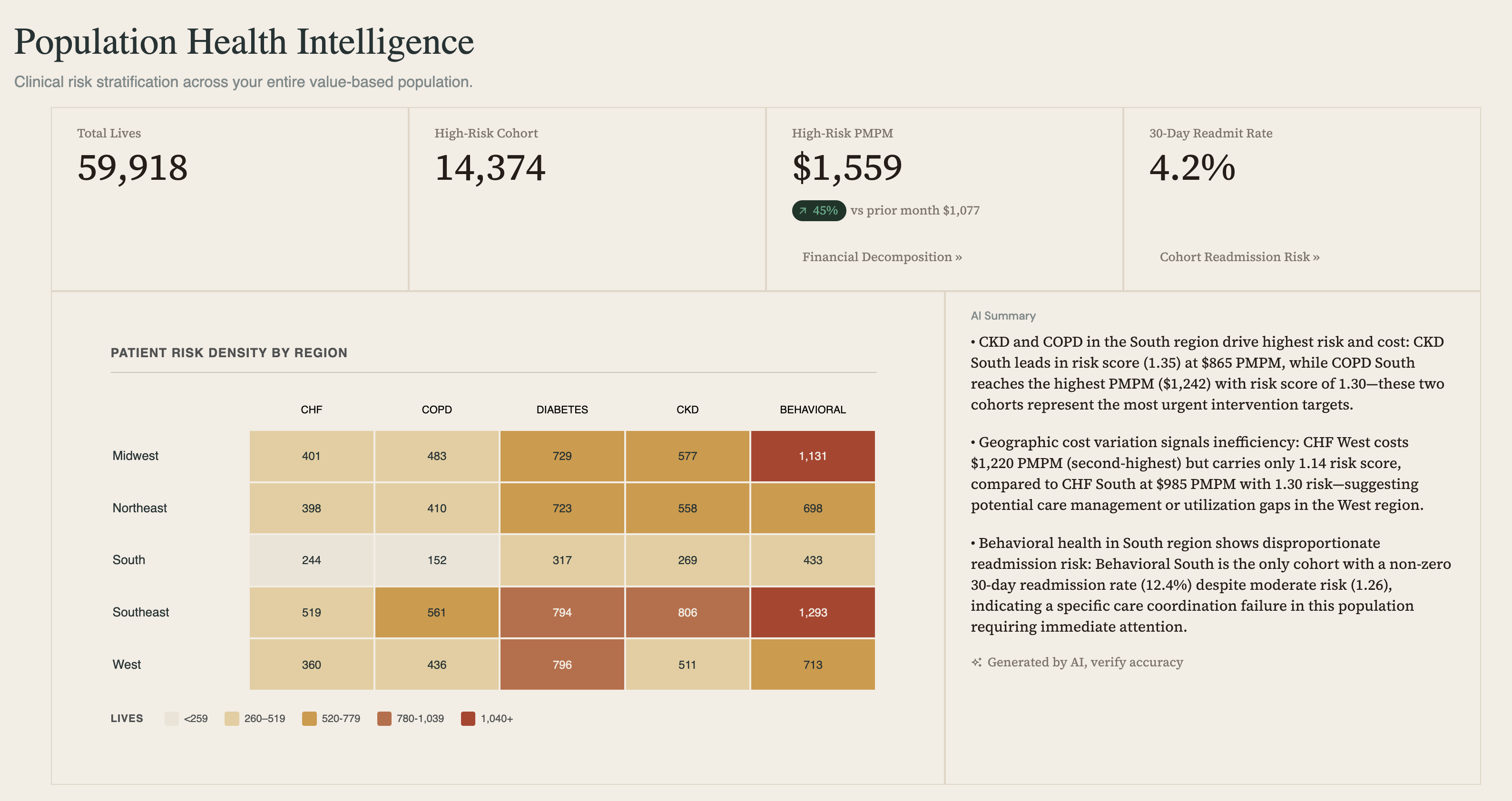
The home page is the whole population at a glance. Across the top are the KPIs that a value-based care team actually answers for: 59,918 total lives, a high-risk cohort of 14,374, a high-risk PMPM of $1,559 (Per Patient Per Month — the average monthly cost a high-risk patient is incurring, up 40% over the prior month), and a 30-day readmission rate of 4.2%.
These aren't static tiles. The interactive dashboard is built in Omni Analytics. Drill-down analyses can be glanced at under Financial Decomposition and Cohort Readmission Risk, for example. The KPIs surfaces the high risk population; the dashboard is the care manager's swiss army knife providing actionable insight.
Below the KPIs is a heat map of regional patient density by condition — CHF, COPD, Diabetes, CKD, and Behavioral across five regions. This is where the workflow actually starts. To its right is a fully integrated AI summary. Using Axiom means your data is secure; it is not traveling to third parties nor being ingested into external tooling.
These are plain-language findings about where risk and cost concentrate. In this snapshot, it's flagging Behavioral dominance in the Midwest and Southeast, as well as, high-cost Diabetes in the Southeast and West. Lastly, similar CKD behaviour is being tracked in the Southeast.
You read the summary, you spot the cells that matter, you click it. Let's follow the highest-cost Behavioral in the Midwest.
Step 2 — Cohort Analysis
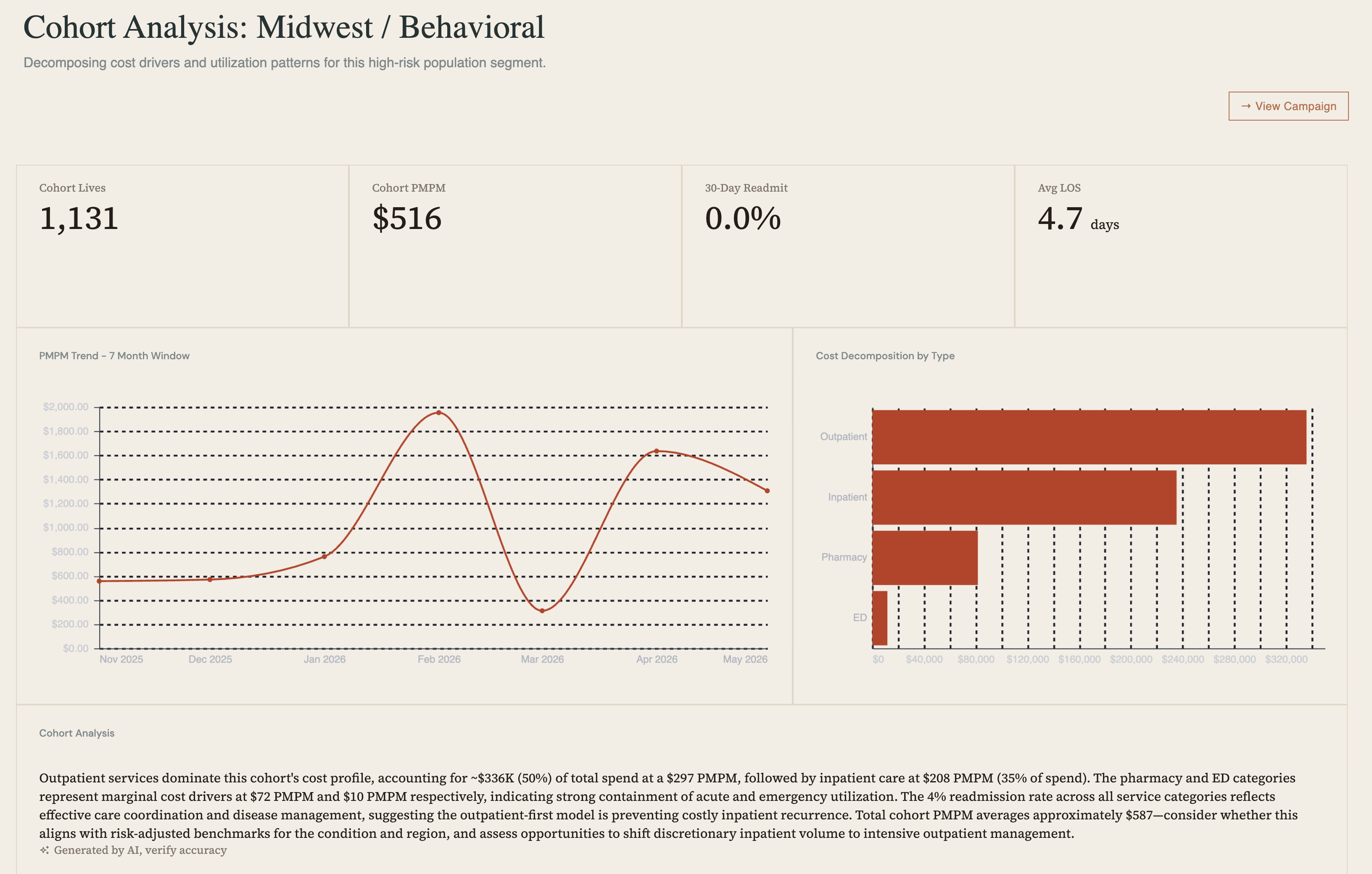
Clicking a heat-map cell lands us on the cohort page for Midwest / Behavioral — 1,131 lives, a cohort PMPM of $516, a 30-day readmission rate of 0.0%, and an average length of stay of 4.7 days. Again, embedded Omni: a PMPM trend over a seven-month window.
At the bottom, note a cost decomposition analysis showing outpatient services driving roughly 50% of total spend. The analysis here is doing real interpretive work, it suggests effective care coordination, and points to available opportunities toward efficient outpatient management.
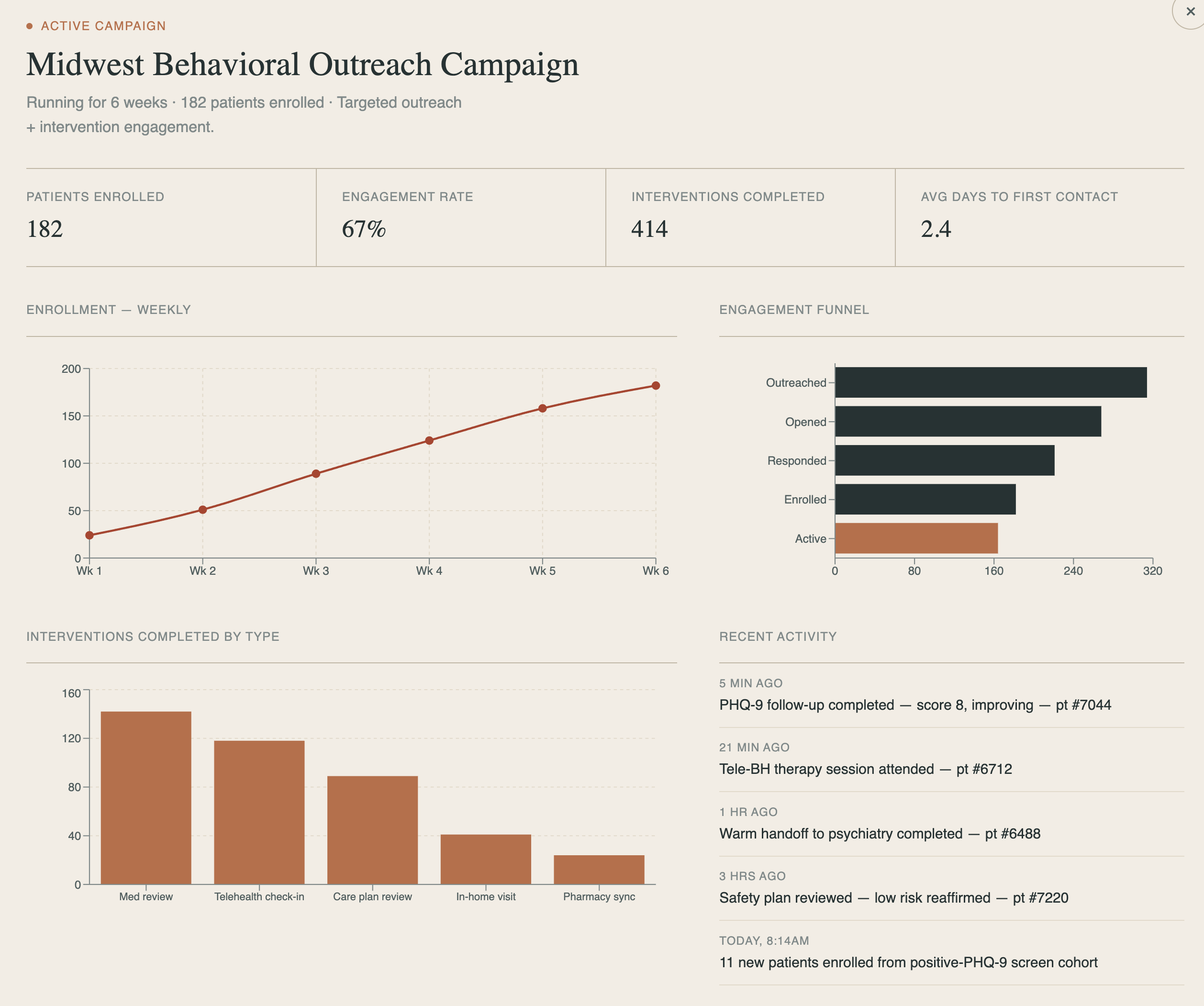
From here you can view an active campaign for this cohort including engagement statistics and analysis details showing campaign efficacy.
Step 3 — The Patient Worklist
The cohort is still 1,131 people. The worklist narrows it to the ones who need attention.
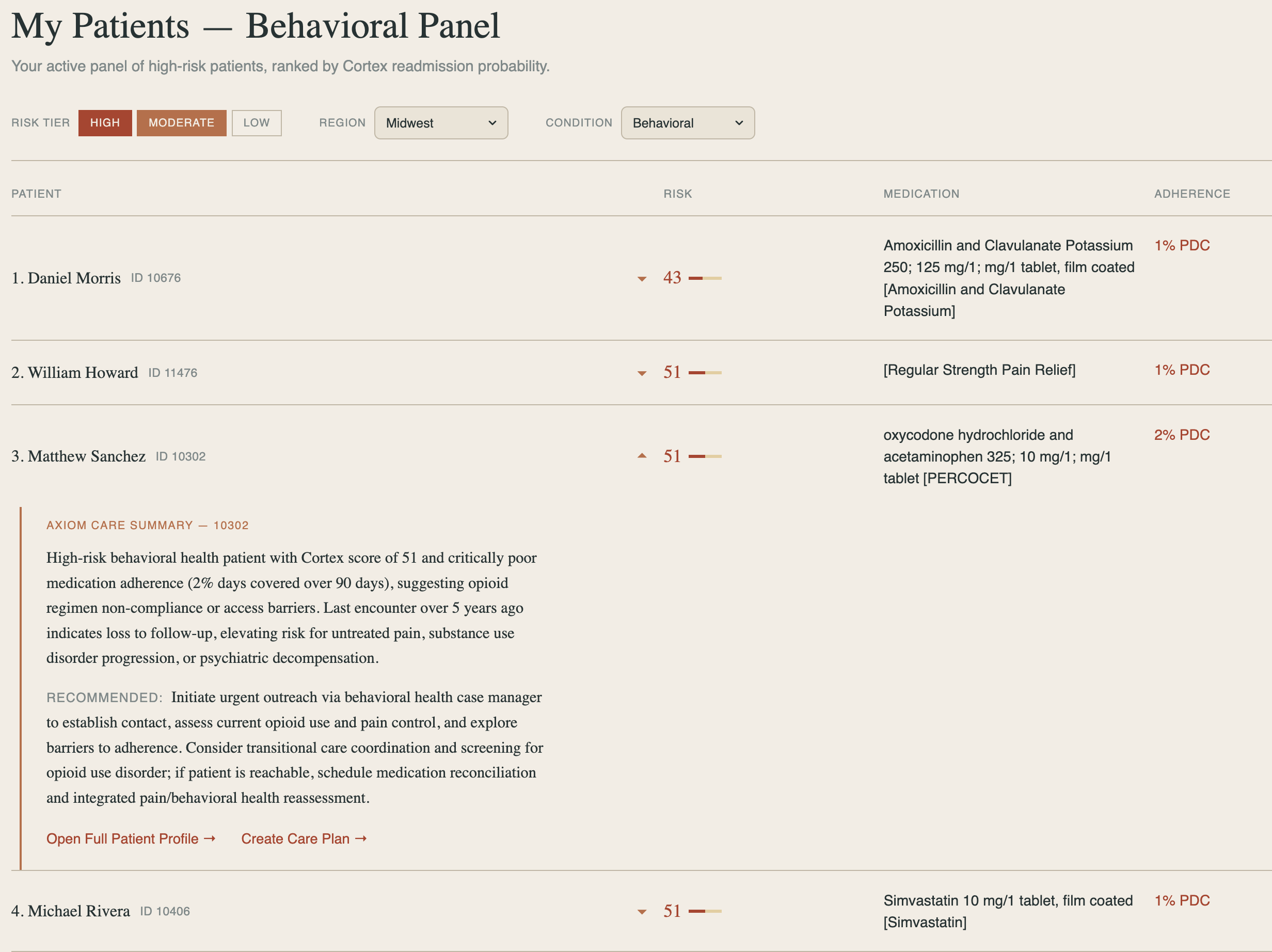
This page is built differently — Omni queries powering a React front end — because the job changed. Up top are filters to isolate exactly the panel you want (risk tier, region, condition). The ranking itself is important: Snowflake Cortex, working with the Tuva Project's readmission data, has scored every patient in the population and surfaced the ones with the highest readmission risk. You're not eyeballing a list.
Click a patient and the Axiom agent activates with a care summary — risk score, medication adherence gaps, clinical context, and a concrete recommended action.
For patient Matthew Sanchez: a Cortex risk score of 51, 2% of days covered on his Behavioral regimen, a critical 5 year primary-care gap, suggesting intentional non-adherence. We also see a recommendation to initiate urgent outreach to assess mental health crisis and coordination for re-engagement to evaluate barriers and current clinical status.
From the summary you can open the full patient profile or start a care plan. The agent tells you what to do next and offers to do it.
Step 4 — The Patient Profile

Following the agent's prompt takes us into the full profile — here, Matthew Sanchez. This is the deep clinical picture: encounter and lab timeline, an Axiom-generated summary of what's driving his risk, and the menu of care-pathway templates and tasks you can assign.
This page is a staging ground between this patient is high-risk and here is the specific path we're putting them on. You can ask Blobby to help identify the readmission drivers and Axiom to prescribe an intervention, then commit the patient to a care queue that blends a template care path with the agent's patient-specific recommendations — which notifies the patient's physician that new tasks are waiting.
Step 5 — The Care Pathway
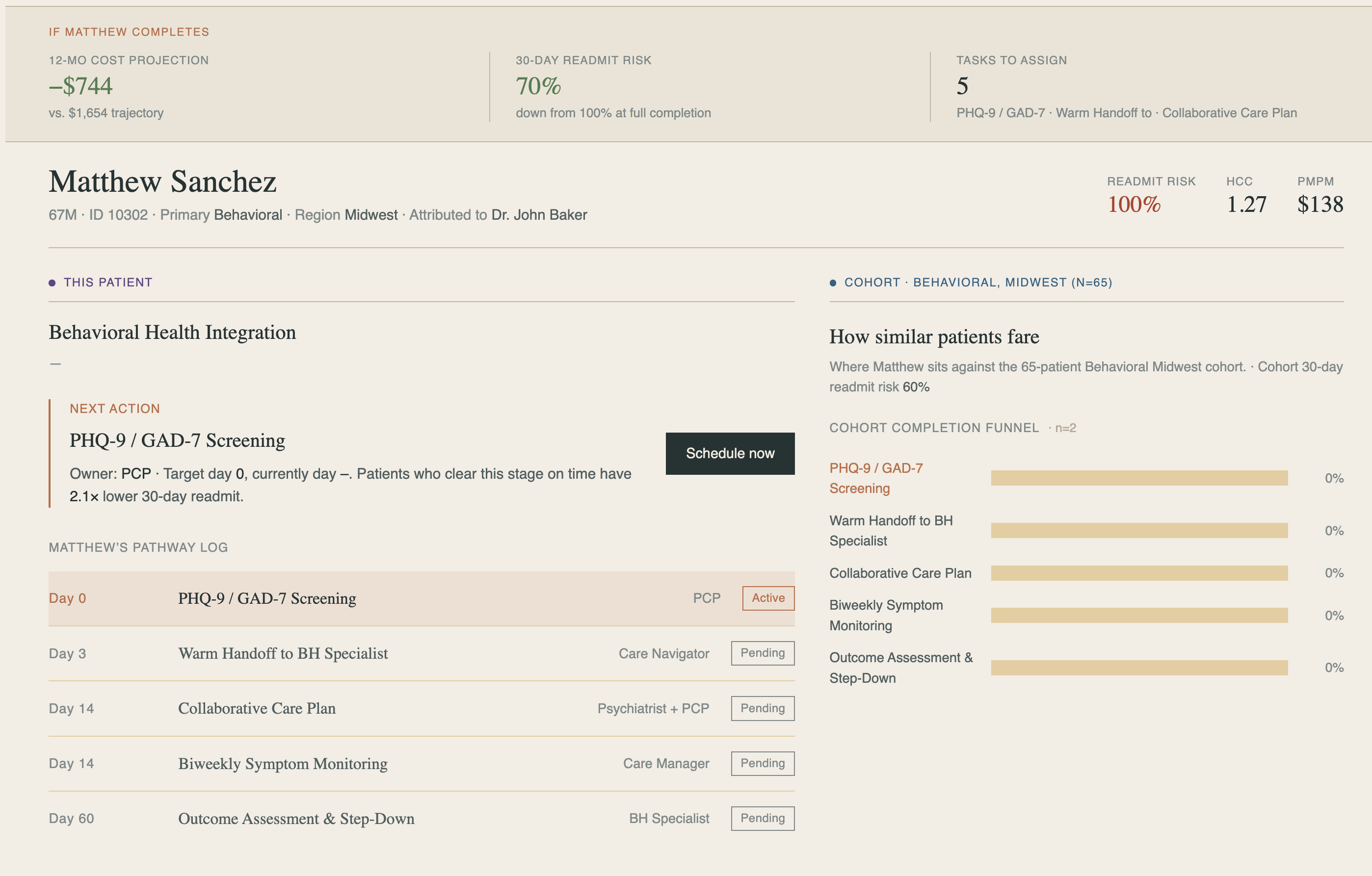
This is where the whole workflow pays off. The Care Pathway page for Matthew Sanchez blends three things on one screen:
- The analytics of acting. A 12-month cost projection of −$744 against trajectory, a 30-day readmission risk down from 100% to 70% at full pathway completion, and a comparison against the Behavioral Midwest cohort — a completion funnel showing where similar patients fall off.
- The prescribed next action. Matthew's pathway log shows a path that has stalled at PHQ-9 / GAD-7 Screening — owned by the primary care practitioner. Patients who clear this stage on time have a 2.1× lower 30-day readmission rate, and the recommended next step is to schedule it now.
- The history and the trajectory. The full log — PHQ-9 / GAD-7 screening, specialist handoff, collaborative care plan, symptom monitoring and, finally, outcome assessment and step down — with what's complete, what's active, and what's pending, including the steps Axiom deployed based on the prior analysis.
One button — Schedule now — takes the action that gets this patient un-stuck. That's the entire arc of the product in a single click: a population of 59,918, narrowed by a model to the patients who matter, narrowed again to the one action that moves a single patient's outcome.
The two-agent idea
Worth pulling out on its own, because it's the design decision that makes Axiom feel different from "a dashboard with a chatbot."
There are two agents working together, not one:
- Blobby is Omni's native agent. Its job is to query. Whenever the application needs an answer from the underlying data, Blobby fires off the query and brings the data back.
- Axiom is powered by Snowflake's Cortex. It is the agent that acts. It takes Blobby's findings and turns them into work under the care manager's direction — creating a cohort campaign, navigating you to the right page, enrolling a patient in a pathway, scheduling the next step, or supplementing the data with documentation and findings from the web.
Reading-the-data and doing-something-about-the-data are genuinely different jobs, and splitting them is why the workflow holds together end to end instead of dead-ending at a chart.
How it was built
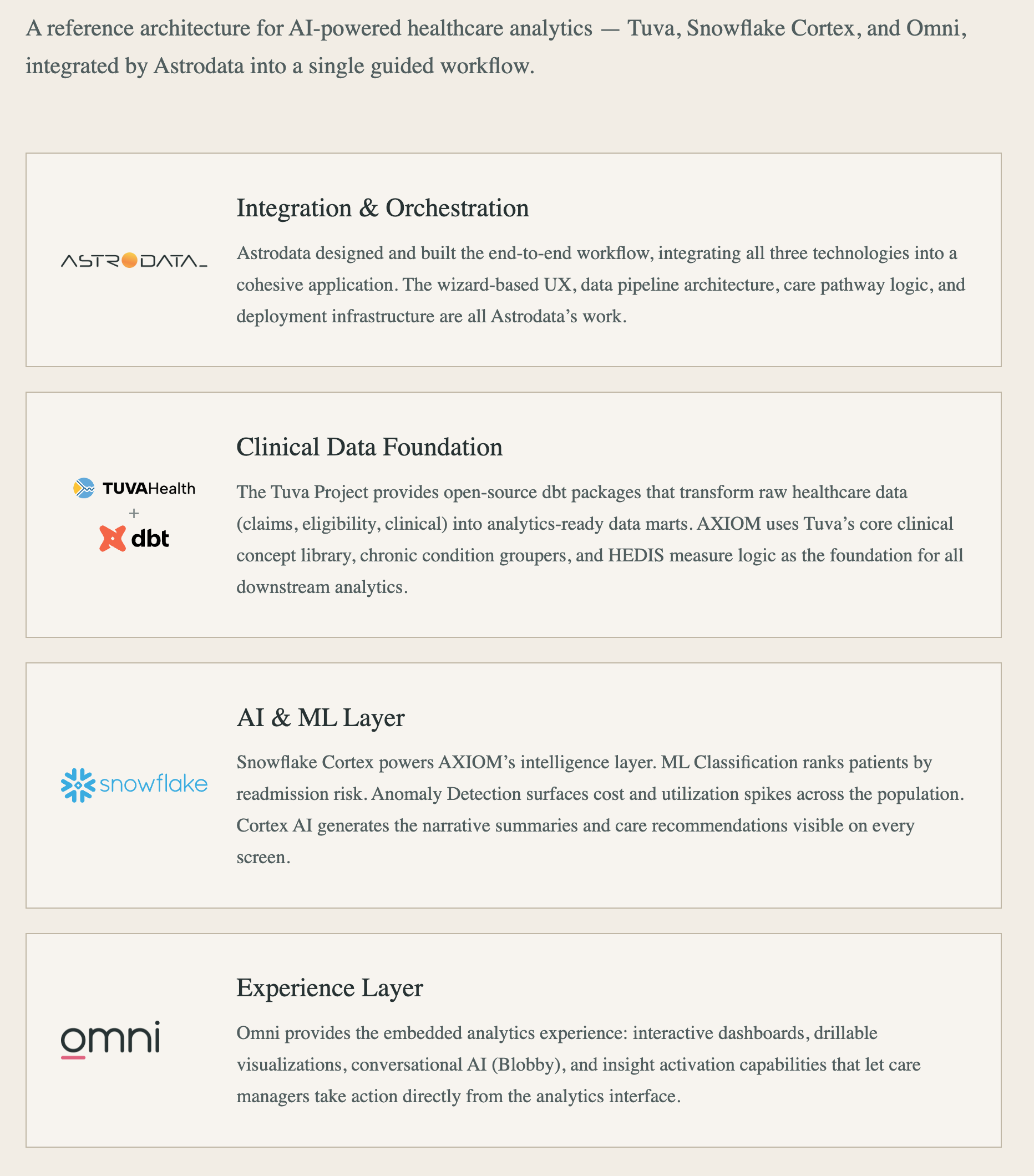
From any page, the How it was Built link opens the reference architecture. Four layers, mapped to the four technologies:
| Layer | Technology | What it does |
|---|---|---|
| Integration & Orchestration | Astrodata | The end-to-end workflow, the React/UX glue, the deployment infrastructure that makes four tools one product. |
| Clinical Data Foundation | The Tuva Project + dbt | Open-source dbt packages that turn raw claims and clinical data into analytics-ready models — clinical concepts, condition groupers, HEDIS measures. |
| AI & ML Layer | Snowflake Cortex | Classifies patients by readmission risk; anomaly detection surfaces cost and utilization spikes; Cortex generates the narrative summaries and recommendations. |
| Experience Layer | Omni | Embedded, interactive, drillable dashboards plus the conversational agent that lets care managers act on the analytics directly. |
Every layer is a tool a healthcare data team can buy and stand up today. Axiom is the proof that a well-integrated solution can deliver a single workflow to drive care-manager productivity. Gone are the days of multiple tools and lost time.
Why this is a reference application
This is a reference application, not a shipped product: It exists to make the architecture concrete. All of these products are enterprise grade, production ready. Omni's embedded analytics, Cortex risk scoring. The open-source Tuva Project is in production at healthcare analytics teams today. The data flowing through all of it is the kind of synthetic clinical data we covered generating in the previous two posts — you can build, demo, and iterate on something like Axiom without moving a single row of PHI into a dev environment.
That's the thread that connects this blog. Generate safe, realistic data → model it with dbt and Tuva → score it with Cortex → surface it through Omni → act on it with an agent. Axiom is what the end of that pipeline looks like.
📈 Next steps
If your organization wants a command center like this on top of your own value-based care data — Snowflake, dbt, Tuva, and Omni integrated into one workflow, with AI assistance wired into the actual work — our team can:
- Stand up the Tuva + dbt clinical data foundation against your source systems.
- Build Cortex risk and readmission models tuned to your population.
- Design the embedded Omni experience and the agent workflows your care managers will use.
- Seed the whole thing with compliant synthetic data so you can build before production is live.
We've built the reference. We'd be glad to build yours. Reach out to talk to an expert.
